

A Novel Prognostic Model Establishment and Treatment Efficacy Analysis for Primary Pulmonary Non-Hodgkin’s Lymphoma
-
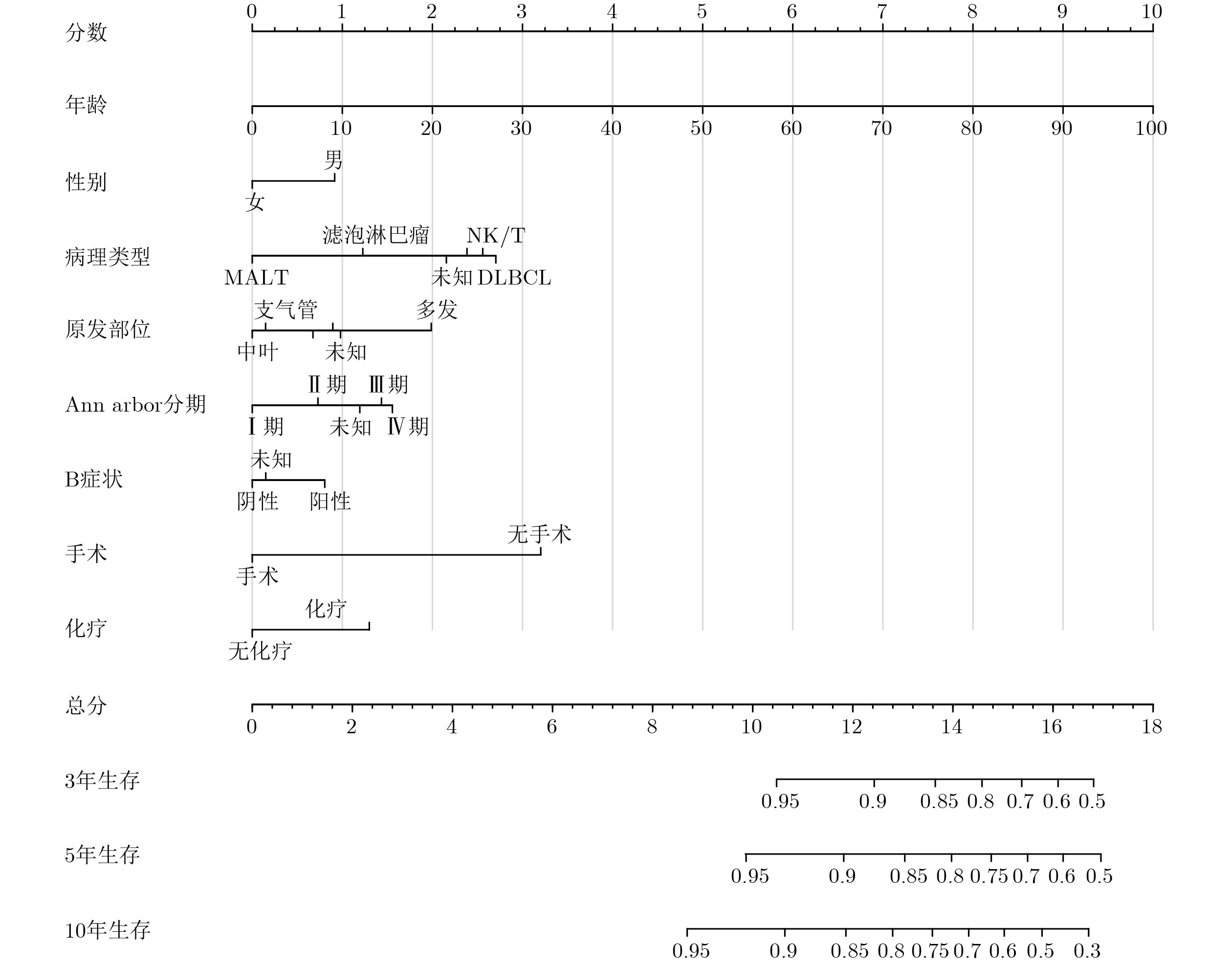
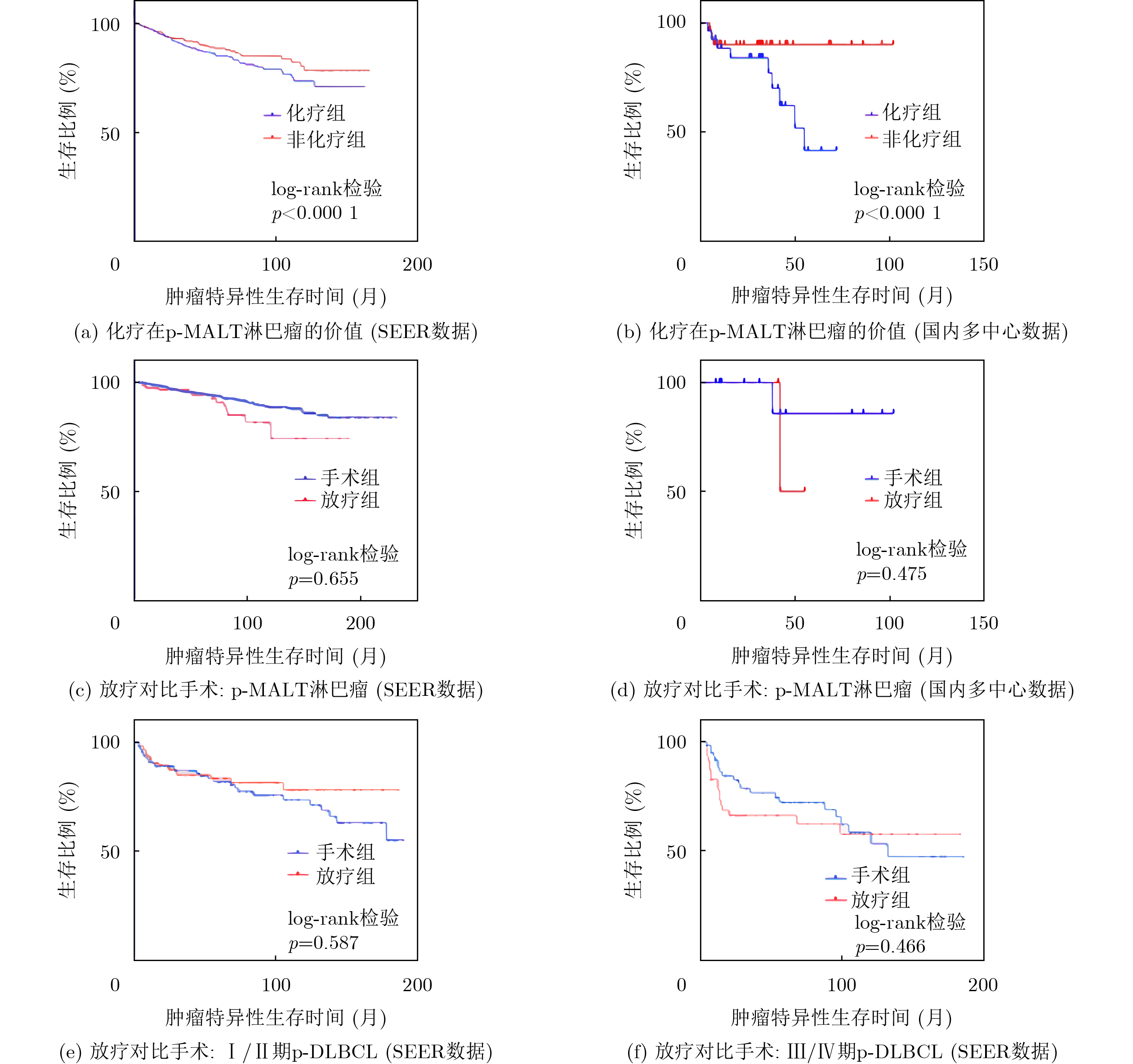
摘要: 该文旨在建立并验证一种新的国际预后指数(IPI),并评估不同治疗方式对原发性肺非霍奇金淋巴瘤(PPL)患者的疗效。该文数据来源于美国癌症数据库(SEER)以及3家中国医院的临床数据库。采用Cox回归分析筛选独立预后因素,并结合列线图和现有IPI模型构建了PPL-IPI,并通过一致性指数(C指数)及校准曲线进行验证。在治疗效果评价中,采用逆概率加权法平衡组间差异,并通过Kaplan-Meier生存曲线及log-rank检验比较不同治疗方式的效果。在SEER数据库中共纳入2000~2019年确诊的4 313例患者,另有2010~2021年确诊的107例来自中国外部验证队列的患者纳入该研究。PPL-IPI模型包含IPI的5个不良因素(年龄>60岁、血清乳酸脱氢酶高、Ann Arbor III/IV期、行为状态评分2~4分和结外侵犯数目超过1个)和Cox模型筛选的4个不良因素:性别(男性)、组织学类型(非黏膜相关淋巴组织(MALT))、B症状(存在)、治疗(未接受),并在原始IPI基础上显著提升预测效能(C-index, 0.932 vs. 0.834)。不同风险组3年生存率分别为:低危组(0~2个因素)96%,低中危组(3~4个因素)82%,高中危组(5个因素)50%,高危组(6~9个因素)11.11%(p<
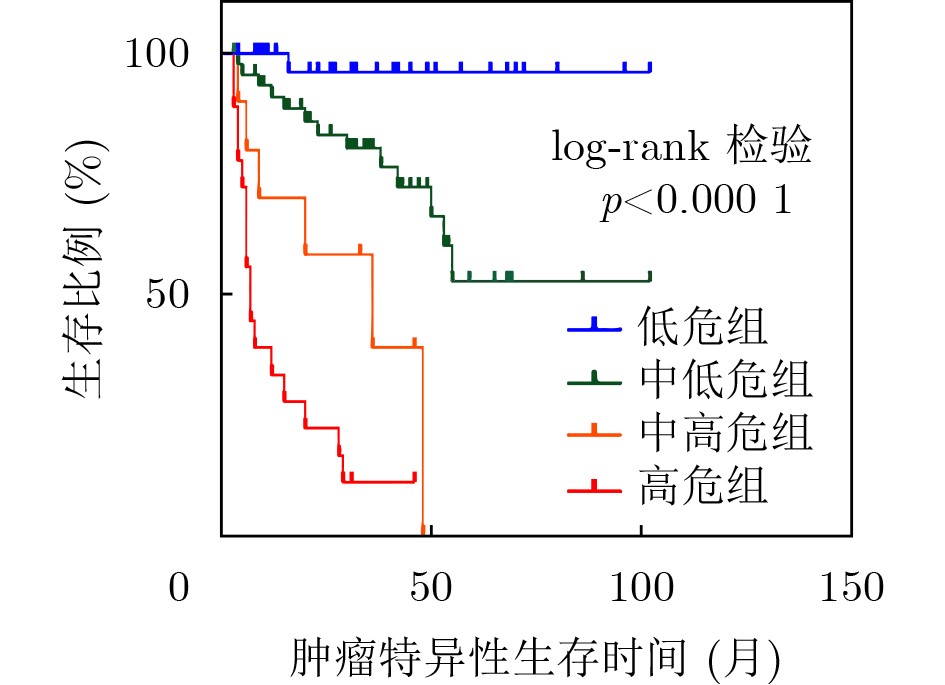
0.000 1 )。在治疗方面,化疗显著降低了原发性肺MALT淋巴瘤患者的肿瘤特异性生存率(p<0.001);手术与放疗在原发性肺MALT淋巴瘤及弥漫大B细胞淋巴瘤患者中的疗效差异均无统计学意义(p>0.05)。结论:基于国际多中心大型队列建立的PPL-IPI具有优异的预后预测能力。对于原发性肺MALT淋巴瘤患者,化疗可能不利于生存;而在原发性肺MALT淋巴瘤和弥漫大B细胞淋巴瘤中,手术和放疗的疗效价值均无显著差别。-
关键词:
- 原发性肺非霍奇金淋巴瘤 /
- 新型预后指数 /
- 疗效分析 /
- 多中心研究 /
- 预后模型
Abstract:Objective At present, few studies have examined Primary Pulmonary non-Hodgkin’s Lymphoma (PPL). Most available reports are single-center retrospective studies. Therefore, no widely accepted prognostic index or treatment strategy for PPL has been established. This study aims to develop and validate a novel prognostic index based on the International Prognostic Index (IPI) for PPL using data from the United States cancer population and Chinese multicenter cohorts. The study also compares the therapeutic effects of different treatment approaches to predict clinical prognosis and provide evidence to support treatment decision-making for PPL. Methods Clinical data from patients diagnosed with PPL were collected from two sources. The first source was the Surveillance, Epidemiology, and End Results (SEER) database of the United States, covering the period from 2000 to 2019. The second source included patients treated between 2010 and 2021 at three tertiary hospitals in China. Independent prognostic factors were identified using the Cox proportional hazards regression model. A nomogram was constructed to predict Cancer-Specific Survival (CSS). Model performance was evaluated using the Concordance index (C-index) and calibration curves. The nomogram was combined with the IPI to develop a novel prognostic index. Risk stratification was performed, and the 3-year Overall Survival (OS) rate was calculated for each risk group. The Inverse Probability of Treatment Weighting (IPTW) method was applied to reduce confounding factors. Survival analysis was conducted using Kaplan-Meier curves and the log-rank test. Results and Discussions A total of 4 313 cases from the SEER database and 107 cases from the Chinese multicenter cohort were included. Multivariate Cox regression analysis showed that independent prognostic factors for PPL included age (p<0.001; Hazard Ratio(HR), 1.078; 95% Confidence Interval(CI), 1.072$ \sim $1.084), Ann Arbor stage (p<0.001), sex (p<0.001; HR, 0.719; 95% CI, 0.624$ \sim $0.829), primary site (p=0.037), pathological type (p< 0.001), B symptoms (p= 0.012; HR, 0.944; 95% CI, 0.773$ \sim $0.997), surgery (p< 0.001; HR, 1.453; 95% CI, 1.221$ \sim $1.728), chemotherapy (p<0.001; HR, 0.742; 95% CI, 0.631$ \sim $0.872), and marital status (p<0.001). Based on these factors, a nomogram predicting 3-, 5-, and 10-year CSS was established. By integrating the nomogram with the IPI, a prognostic model for PPL was developed with a C-index of 0.932. Using defined risk parameters, a novel prognostic index for PPL was constructed. The risk parameters included age>60 years, Ann Arbor stage III/IV, serum Lactate DeHydrogenase (LDH) level>1 times the normal level, performance status score>2, number of extranodal sites>1, male sex, pathological type other than Mucosa-Associated Lymphoid Tissue (MALT) lymphoma, presence of B symptoms, and absence of cancer treatment. Risk stratification was defined as follows: low-risk group (0$ \sim $2 risk factors), low-intermediate-risk group (3$ \sim $4 risk factors), high-intermediate-risk group (5 risk factors), and high-risk group (6$ \sim $9 risk factors). The corresponding 3-year OS rates were 96.97%, 82.61%, 50.00%, and 11.11%, respectively (p<0.000 1). In the analysis of treatment efficacy, both the United States and Chinese datasets showed that chemotherapy significantly reduced CSS in patients with primary pulmonary MALT lymphoma (p<0.001). No significant difference was observed between surgery and radiotherapy in patients with either primary pulmonary MALT lymphoma or diffuse large B-cell lymphoma (p>0.05). Conclusions This study develops a novel prognostic index for PPL based on data from the United States cancer population and a Chinese multicenter cohort. The model includes age, disease stage, serum LDH level, performance status score, and number of extranodal sites. The index demonstrates strong predictive performance and accuracy. Risk stratification based on this index provides estimated 3-year OS rates for different risk groups. Treatment efficacy analysis indicates that chemotherapy may reduce CSS in patients with primary pulmonary MALT lymphoma. In addition, no significant difference is observed between surgery and radiotherapy in patients with primary pulmonary MALT lymphoma or diffuse large B-cell lymphoma. -
表 1 基于SEER数据库的原发性肺淋巴瘤患者的基线特征及预后因素的单因素与多因素Cox分析
参数 例数( 4 313 例)比例(%) 单因素Cox回归 多因素Cox回归 p值 HR 95%CI p值 HR 95%CI 年龄(岁) 65.6 - <0.001 1.034 1.028 1.039 <0.001 1.078 1.072 1.084 性别(男性) 1944 45.1 0.001 0.804 0.705 0.918 <0.001 0.719 0.624 0.829 原发部位 0.001 0.037 主支气管 146 3.4 对照 对照 上叶 1226 28.4 0.177 0.207 中叶 329 7.6 0.002 0.664 0.514 0.859 0.022 0.694 0.507 0.950 下叶 1137 26.4 0.637 0.402 多发 86 2.0 0.013 1.195 1.039 1.374 0.790 1.470 0.956 2.262 未知 1389 32.2 0.137 0.825 组织学类型 <0.001 <0.001 NK/T细胞 390 9.0 对照 对照 DLBCL 1321 30.6 0.003 1.366 1.109 1.684 0.578 1.083 0.817 1.437 滤泡 178 4.1 0.036 0.718 0.527 0.979 0.046 0.648 0.422 0.993 MALT 1686 39.1 <0.001 0.383 0.302 0.486 <0.001 0.409 0.304 0.550 未知 607 14.1 0.129 0.362 确诊依据为病理 3560 82.5 0.003 0.748 0.619 0.905 0.677 0.958 0.782 1.173 Ann Arbor 分期 <0.001 <0.001 I期 1646 38.2 对照 对照 II期 588 13.6 <0.001 1.260 1.061 1.386 0.022 1.315 1.041 1.662 III期 167 3.9 0.355 <0.001 1.567 1.284 1.913 IV期 918 21.3 0.011 1.463 1.091 1.961 <0.001 1.773 1.293 2.432 未知 994 23.0 0.186 <0.001 1.714 1.351 2.174 B症状 <0.001 0.012 阳性 468 10.9 对照 对照 阴性 1992 46.2 <0.001 0.768 0.698 0.845 0.042 0.944 0.773 0.997 未知 1853 43.0 <0.001 1.277 1.128 1.445 0.573 手术 1306 30.3 <0.001 1.467 1.350 1.593 <0.001 1.453 1.221 1.728 放疗 580 13.4 0.266 0.948 0.863 1.041 化疗 2010 46.6 <0.001 0.734 0.686 0.786 <0.001 0.742 0.631 0.872 婚姻状态 <0.001 <0.001 丧偶 660 15.3 对照 对照 离异 408 9.5 0.093 0.808 0.630 1.036 0.048 0.747 0.559 0.997 已婚 2380 55.2 0.024 0.789 0.642 0.970 0.007 0.627 0.448 0.879 单身 611 14.2 0.490 0.565 未知 254 5.9 0.010 0.859 0.765 0.965 <0.001 0.680 0.564 0.819 第1原发 3321 77.0 0.036 1.088 1.005 1.176 0.932 注:HR/CI仅对显著项展示,参照组与不显著项不展示。  下载: 导出CSV
下载: 导出CSV
表 2 多中心外部验证队列中原发性肺淋巴瘤患者的基线特征
参数 例数(107例) 比例(%) 年龄(<60岁) 51 47.7 性别(男性) 61 57.0 原发部位 主支气管 4 3.7 上叶 31 29.0 中叶 14 13.1 下叶 14 13.1 多发 37 34.6 未知 7 6.5 组织学类型 NK/T细胞 7 6.5 DLBCL 29 27.1 滤泡 2 1.9 MALT 57 53.3 未知 8 7.5 Ann Arbor分期 I/II期 48 44.9 III/IV期 48 44.9 未知 11 10.2 B症状 阳性 41 38.3 阴性 52 48.6 未知 14 13.1 手术 27 25.2 放疗 19 17.8 化疗 62 57.9 血清LDH水平,正常 82 76.6 行为状态评分<2 96 89.7 结外侵犯数目>1 31 29.0
下载: 导出CSV
表 3 原发性肺非霍奇金淋巴瘤新型预后指数的定义与3年总生存率
参数 定义 3年生存率(%) 危险因素 年龄 >60岁 血清LDH水平 >正常 Ann Arbor分期 III/IV期 行为状态评分 2~4分 结外侵犯数目 >1 性别 男性 组织学类型 除MALT外 B症状 阳性 抗肿瘤治疗 未治疗 危险分层 低危组 0~2 96.97 中低危组 3~4 82.61 中高危组 5 50.00 高危组 6~9 11.11
下载: 导出CSV
-
[1] SIEGEL R L, MILLER K D, FUCHS H E, et al. Cancer statistics, 2022[J]. CA: A Cancer Journal for Clinicians, 2022, 72(1): 7–33. doi: 10.3322/caac.21708. [2] SMALL W. Perez and brady’s principles and practice of radiation oncology[J]. JAMA, 2009, 301(19): 2046–2051. doi: 10.1001/jama.2009.718. [3] GIZA A, DUMNICKA P, KALICIŃSKA E, et al. Retrospective analysis of primary pulmonary lymphoma cases from Polish Lymphoma Research Group centers reveals associations between initial symptoms and outcomes[J]. Scientific Reports, 2025, 15(1): 27883. doi: 10.1038/s41598-025-12469-7. [4] PDQ Pediatric Treatment Editorial Board. Childhood non-hodgkin lymphoma treatment (PDQ®)-Health professional version[R]. Bethesda: National Cancer Institute, 2002. [5] SMYTH R, SLOAN J M, BURKS E, et al. Primary pulmonary marginal zone lymphoma: An unusual cause of pulmonary infiltrates[J]. Respirology Case Reports, 2021, 9(8): e00806. doi: 10.1002/rcr2.806. [6] DONG Congsong, XIA Peng, QIU Wenli, et al. Evaluation of CT features for differentiating consolidation pattern of pulmonary MALT lymphoma from pneumonic-type lung adenocarcinoma[J]. Frontiers in Oncology, 2023, 13: 1234291. doi: 10.3389/fonc.2023.1234291. [7] The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma[J]. The New England Journal of Medicine, 1993, 329(14): 987–994. doi: 10.1056/NEJM199309303291402. [8] HE Xiaoyu, HUANG Qian, LI Wenqiang, et al. Prognostic factors and predictive models for primary pulmonary diffuse large B-cell lymphoma: A population-based analysis[J]. Hematology, 2024, 29(1): 2420160. doi: 10.1080/16078454.2024.2420160. [9] THIEBLEMONT C, CASCIONE L, CONCONI A, et al. A MALT lymphoma prognostic index[J]. Blood, 2017, 130(12): 1409–1417. doi: 10.1182/blood-2017-03-771915. [10] KIM H D, CHO H, JEONG H, et al. A prognostic index for extranodal marginal-zone lymphoma based on the mucosa-associated lymphoid tissue International Prognostic Index and serum β2-microglobulin levels[J]. British Journal of Haematology, 2021, 193(2): 307–315. doi: 10.1111/bjh.17222. [11] SHEN Hui and ZHOU Yaodong. Clinical features and surgical treatment of primary pulmonary lymphoma: A retrospective study[J]. Frontiers in Oncology, 2022, 12: 779395. doi: 10.3389/fonc.2022.779395. [12] NING Ye, HE Haiyan, LI Qiuyuan, et al. The prognosis of patients with primary pulmonary mucosa-associated lymphoid tissue lymphoma: Treated with surgery or chemotherapy?[J]. European Journal of Cardio-Thoracic Surgery, 2024, 65(3): ezae064. doi: 10.1093/ejcts/ezae064. [13] VANDEN EYNDEN F, FADEL E, DE PERROT M, et al. Role of surgery in the treatment of primary pulmonary B-cell lymphoma[J]. The Annals of Thoracic Surgery, 2007, 83(1): 236–240. doi: 10.1016/j.athoracsur.2006.08.026. [14] ABRISQUETA P. New insights into first-line therapy in diffuse large B-cell lymphoma: Are we improving outcomes?[J]. Journal of Clinical Medicine, 2024, 13(7): 1929. doi: 10.3390/jcm13071929. [15] JELICIC J, JUUL-JENSEN K, BUKUMIRIC Z, et al. Prognostic indices in diffuse large B-cell lymphoma: A population-based comparison and validation study of multiple models[J]. Blood Cancer Journal, 2023, 13(1): 157. doi: 10.1038/s41408-023-00930-7. [16] CLAVIJO N D, AGUIRRE J C F, DEL PILAR AGUDELO LOPEZ C, et al. Aligning outcomes: DLBCL prognosis at a 4th Level University Hospital in Bogotá is comparable to high-income nations, identification of additional prognostic markers for overall survival and relapse[J]. Ecancermedicalscience, 2024, 18: 1717. doi: 10.3332/ecancer.2024.1717. [17] PENCINA M J and D'AGOSTINO R B. Overall C as a measure of discrimination in survival analysis: Model specific population value and confidence interval estimation[J]. Statistics in Medicine, 2004, 23(13): 2109–2123. doi: 10.1002/sim.1802. [18] KAMMULA A V, SCHÄFFER A A, RAJAGOPAL P S, et al. Outcome differences by sex in oncology clinical trials[J]. Nature Communications, 2024, 15(1): 2608. doi: 10.1038/s41467-024-46945-x. [19] KISERUD C E, SCHOVER L R, DAHL A A, et al. Do male lymphoma survivors have impaired sexual function?[J]. Journal of Clinical Oncology, 2009, 27(35): 6019–6026. doi: 10.1200/JCO.2009.23.2280. [20] SOLAL-CÉLIGNY P, ROY P, COLOMBAT P, et al. Follicular lymphoma international prognostic index[J]. Blood, 2004, 104(5): 1258–1265. doi: 10.1182/blood-2003-12-4434. [21] O'REILLY S E and CONNORS J M. Non-Hodgkin’s lymphoma. I: Characterisation and treatment[J]. British Medical Journal, 1992, 304(6843): 1682–1686. doi: 10.1136/bmj.304.6843.1682. [22] RADERER M, KIESEWETTER B, and FERRERI A J M. Clinicopathologic characteristics and treatment of marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma)[J]. CA: A Cancer Journal for Clinicians, 2016, 66(2): 153–171. doi: 10.3322/caac.21330. [23] CADRANEL J, WISLEZ M, and ANTOINE M. Primary pulmonary lymphoma[J]. European Respiratory Journal, 2002, 20(3): 750–762. doi: 10.1183/09031936.02.00404102. [24] GRAHAM B B, MATHISEN D J, MARK E J, et al. Primary pulmonary lymphoma[J]. The Annals of Thoracic Surgery, 2005, 80(4): 1248–1253. doi: 10.1016/j.athoracsur.2005.04.014. [25] ZUCCA E and CAVALLI F. Extranodal lymphomas[J]. Annals of Oncology, 2000, 11(S3): 219–222. doi: 10.1093/annonc/11.suppl_3.219. [26] WANG Haotian, ZHANG Ying, LI Zhaoxia, et al. Characteristics, efficacy, and prognosis analysis of newly diagnosed marginal zone lymphoma[J]. Frontiers in Immunology, 2024, 15: 1466859. doi: 10.3389/fimmu.2024.1466859. [27] ZIEPERT M, HASENCLEVER D, KUHNT E, et al. Standard international prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era[J]. Journal of Clinical Oncology, 2010, 28(14): 2373–2380. doi: 10.1200/JCO.2009.26.2493. [28] SEHN L H and GASCOYNE R D. Diffuse large B-cell lymphoma: Optimizing outcome in the context of clinical and biologic heterogeneity[J]. Blood, 2015, 125(1): 22–32. doi: 10.1182/blood-2014-05-577189. [29] MAZLOOM A, MEDEIROS L J, MCLAUGHLIN P W, et al. Marginal zone lymphomas: Factors that affect the final outcome[J]. Cancer, 2010, 116(18): 4291–4298. doi: 10.1002/cncr.25325. [30] PARRY-JONES N, MATUTES E, GRUSZKA-WESTWOOD A M, et al. Prognostic features of splenic lymphoma with villous lymphocytes: A report on 129 patients[J]. British Journal of Haematology, 2003, 120(5): 759–764. doi: 10.1046/j.1365-2141.2003.04165.x. [31] ZHOU Zheng, SEHN L H, RADEMAKER A W, et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era[J]. Blood, 2014, 123(6): 837–842. doi: 10.1182/blood-2013-09-524108. [32] ZELENETZ A D, GORDON L I, CHANG J E, et al. NCCN Guidelines® insights: B-cell lymphomas, version 5.2021[J]. Journal of the National Comprehensive Cancer Network, 2021, 19(11): 1218–1230. doi: 10.6004/jnccn.2021.0054. [33] TIAN Zhizhong, LIU Linxia, WU Lijuan, et al. Correction: Enhancement of vitamin B6 production driven by omics analysis combined with fermentation optimization[J]. Microbial Cell Factories, 2024, 23(1): 257. doi: 10.1186/s12934-024-02532-9. [34] PINOTTI G, ZUCCA E, ROGGERO E, et al. Clinical features, treatment and outcome in a series of 93 patients with low-grade gastric MALT lymphoma[J]. Leukemia & Lymphoma, 1997, 26(5/6): 527–537. doi: 10.3109/10428199709050889. [35] THIEBLEMONT C, DUMONTET C, BOUAFIA F, et al. Outcome in relation to treatment modalities in 48 patients with localized gastric MALT lymphoma: A retrospective study of patients treated during 1976-2001[J]. Leukemia & Lymphoma, 2003, 44(2): 257–262. doi: 10.1080/1042819021000035680. [36] LIAO Qiuling, YU Qilin, YU Cheng, et al. Pulmonary mucosa-associated lymphoid tissue lymphoma: Insights from a 15-year study at a single institution involving 14 clinical cases[J]. World Journal of Surgical Oncology, 2024, 22(1): 219. doi: 10.1186/s12957-024-03500-8. [37] ZUCCA E and BERTONI F. The spectrum of MALT lymphoma at different sites: Biological and therapeutic relevance[J]. Blood, 2016, 127(17): 2082–2092. doi: 10.1182/blood-2015-12-624304. [38] TSANG R W and GOSPODAROWICZ M K. Radiation therapy for localized low-grade non-Hodgkin’s lymphomas[J]. Hematological Oncology, 2005, 23(1): 10–17. doi: 10.1002/hon.743. [39] WÖHRER S, TROCH M, STREUBEL B, et al. MALT lymphoma in patients with autoimmune diseases: A comparative analysis of characteristics and clinical course[J]. Leukemia, 2007, 21(8): 1812–1818. doi: 10.1038/sj.leu.2404782. [40] BORIE R, WISLEZ M, ANTOINE M, et al. Lymphoproliferative disorders of the lung[J]. Respiration, 2017, 94(2): 157–175. doi: 10.1159/000477740. [41] ARMSTRONG P, HAYDEN P, JEFFERS M, et al. Pulmonary mucosa-associated lymphoid tissue lymphoma treated with radiation therapy: A case report and review of the literature[J]. Case Reports in Oncology, 2023, 16(1): 1528–1535. doi: 10.1159/000534802. [42] SANGUEDOLCE F, ZANELLI M, ZIZZO M, et al. Primary pulmonary B-cell lymphoma: A review and update[J]. Cancers, 2021, 13(3): 415. doi: 10.3390/cancers13030415. [43] FERRARO P, TRASTEK V F, ADLAKHA H, et al. Primary non-Hodgkin's lymphoma of the lung[J]. The Annals of Thoracic Surgery, 2000, 69(4): 993–997. doi: 10.1016/s0003-4975(99)01535-0. [44] REZAZADEH A, SZABO A, KHURANA A, et al. Outcomes of limited stage primary bone diffuse large B-cell lymphoma in the rituximab era: A multicenter, retrospective study[J]. Haematologica, 2024, 109(5): 1439–1444. doi: 10.3324/haematol.2023.283210. [45] KIEŁBOWSKI K, KORDYKIEWICZ D, JESIONKA J, et al. A rare case of primary pulmonary diffuse large B-cell lymphoma transformed from marginal zone mucosa-associated lymphoid tissue lymphoma[J]. Medicina, 2024, 60(6): 840. doi: 10.3390/medicina60060840. -


 下载:
下载:


图(4) / 表(3)
计量
- 文章访问数: 371
- HTML全文浏览量: 279
- PDF下载量: 35
- 被引次数: 0
